A 80 yo man is brought from an assisted-living facility because of fever, productive cough, tachycardia and dyspnoea.
He has a history of dementia and hypertension.
He is cachectic, you hear ronchi on the left side.
How should you approach this patient?
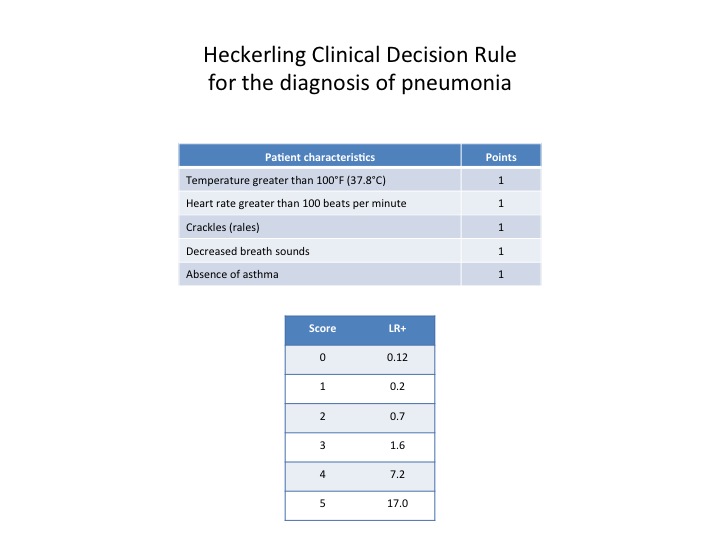
In the Emergency department setting the pretest probability of pneumonia is 15%
It’s far in time when Laennec said that with the stethoscope doctors would have made a definitive diagnosis of pneumonia in every patient (1819).
In this case the presence of 4/5 clinical findings increases the probability of 40%, it is not bad, but it depends on pretest probability.
Any combination of clinical findings is not usefull to rule in or out the diagnosis of pneumonia, to confirm this you need a chest radiography….
but what if it is negative?
Post test probability after negative supine X Ray
A negative supine Chest X-Ray reduces the probability of pneumonia a little: about a 20%.
Is it the time for a combined imaging strategy?
Conclusion
The supine position X-Ray, with a single anteroposterior view has a poor performance. If you are an ECO-expert try to perform an ultrasound at the bedside. Maybe you’ll find a focused interstitial syndrome, or subpleural consolidation. If negative you can feel comfortable. Practice make perfect!!!
When the CT? when the diagnosis is unclear, or when you suspect any complication.
Bibliography
Clinical prediction rule for pulmonary infiltrates.
Ann Intern Med 1990; 113 (9):664-670.
PS Heckerling et al.
Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination.
JAMA. 1997;278:1440–5.
JP Methlay et al.
Lung ultrasound is an accurate diagnostic tool for thw diagnosis of pneumonia in the emergency department.
Emerg Med J 2012; 29 19-23.
F. Cortellaro et al.