I t’s a dark night when a red code arrive at the ED by ambulance. Paramedics tell you: “called for acute dyspnoea, I think it’s a COPD exacerbation, he is wheezing, I gave him bronchodilators and steroids, but he is worsening”. He has a history of COPD and hypertension. He presents sweaty, dyspneic, arterial pressure is high (220/110). Physical examination is normal except for wheezing.
What is the LR of clinical signs in the diagnosis of pulmonary oedema?
Conclusion
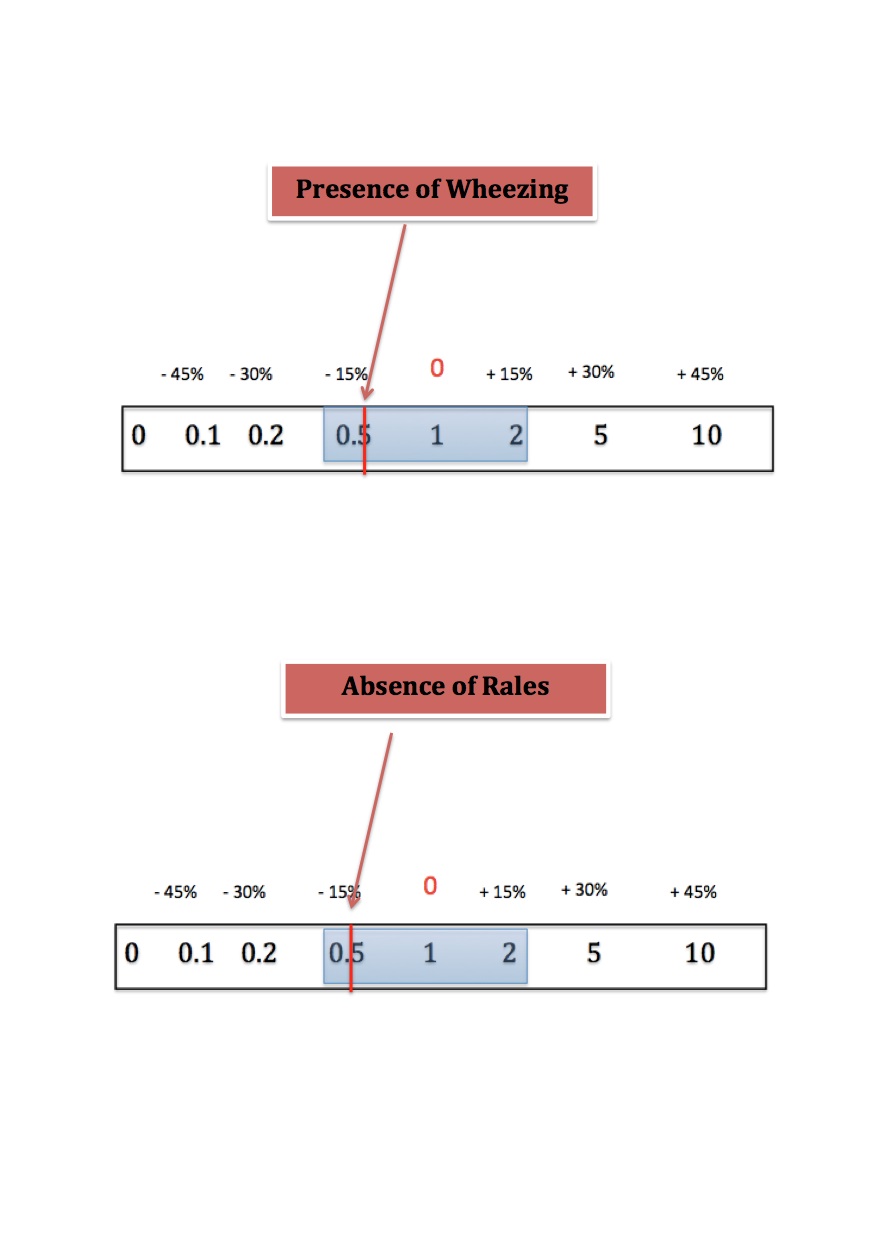
The absence of pulmonary rales (sensitivity 0.60; specificity 0,78; LR + 2,73 LR – 0,51) and the presence of wheezing (sensitivity 0.22; specificity 0,58; LR+ 0,52 LR – 1,34) decreased the likelihood of heart failure insufficently to rule out a pulmonary oedema in a patient presenting with acute dyspnoea.
In acute setting you might need something more than your stetoscope
….but is it x ray?
Bibliography
Does this dyspneic patient in the emergency department have congestive heart failure?
Wang CS, FitzGerald JM, Schulzer M, Mak E, Ayas NT. Department of Medicine, University of British Columbia, Canada.JAMA. 2005 Oct 19;294(15):1944-56.