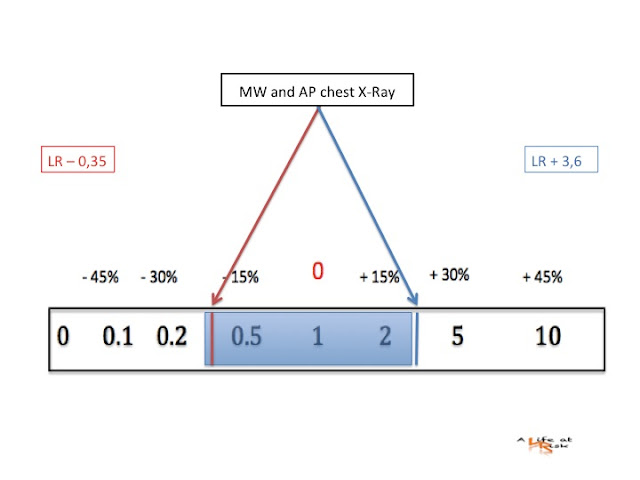
A 70 yo man come to the ED for restrosternal chest pain and shortness of breath during minimal activity in the last days. He is an ex smoker, with a history of hypertension. On physical examination the patient is not in distress, with a regular blood pressure and regular oximetry. ECG shows no evidence of ischemia. You first think about coronary artery disease, but you also want to exclude an aortic dissection. In Radiology the patient remaine seated and receive an anteroposterior (AP) chest Xray: maximal mediastinal width (MW) is 8,80 cm (the optimal cutoff level is 8,65 cm), no other signs.
Shall you worry?
Conclusion
Chest X-Ray is often the initial test in a suspect of thoracic aortic dissection. It is not the definitive test for aortic disease, but it’s use is justified by detection of other causes of chest pain and for the low risk patient.
The widening of the mediastinum is the first finding of an aortic dissection, but the accuracy of diagnostic measurements is different between antero-posterior (AP) and postero-anterior (PA) chest-Xray, in fact the standard focal film distance is easy to obtain if the patient is on PA projection, but if the patient is supine or sitting the diagnostic accuracy is lower and it is also impossible to obtain a lateral projection.
So… get up, stand up…. if you can!
Bibliography
Emerg Radiol. 2012 Mar 14.
Diagnostic accuracy of mediastinal width measurement on posteroanterior and anteroposterior chest radiographs in the depiction of acute nontraumatic thoracic aortic dissection.
Lai V, Tsang WK, Chan WC, Yeung TW.