I t’s a dark night when a red code arrive at the ED by ambulance.
Paramedics tell you: “called for acute dyspnoea, I think it’s a COPD exacerbation, he is wheezing, I gave him bronchodilators and steroids, but he is worsening”.
He has a history of COPD and hypertension.
He presents sweaty, dyspneic, arterial pressure is high (220/110).
Physical examination is normal except for wheezing.
AP Chest x ray shows no signs of congestion.
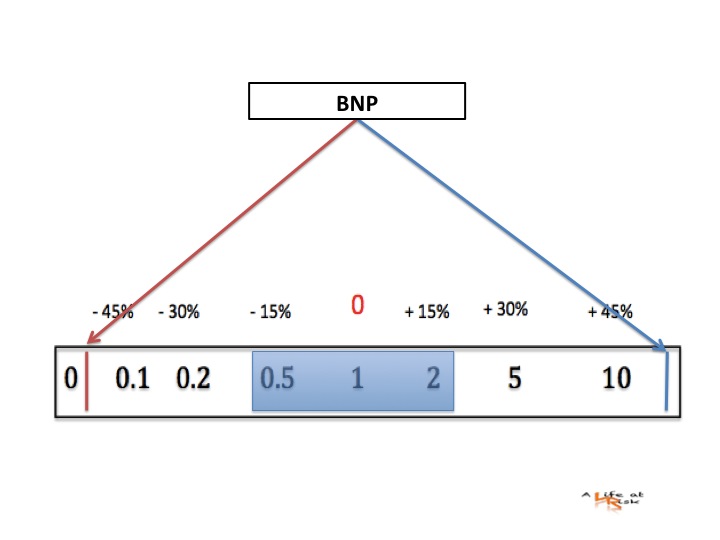
What about BNP?
Conclusion
Natriuretic peptides have a very high negative predictive value that allows us to rule out dyspnoea of cardiogenic origin when values are normal. However, there are several circumstances in which natriuretic peptides may be elevated for other reasons, and data may be confounded. Thus, especially in cases where NT-proBNP levels are only slightly abnormal, the “grey zone”, echographic assessment of pulmonary congestion could help in the management of patients with dyspnoea.
Moreover, natriuretic peptide analysis is not always available, especially in peripheral emergency departments, as it requires specialised laboratory equipment. If the assay is not available, ULCs may offer a plausible alternative. In patients admitted with acute dyspnoea, pulmonary congestion, sonographically imaged as ULCs, is significantly correlated to NT-proBNP values
Bibliography
L. Gargani a, F. Frassi a , G. Soldati b , P. Tesorio c , M. Gheorghiade d , E. Picano a
Ultrasound lung comets for the differential diagnosis of acute cardiogenic dyspnoea: A comparison with natriuretic peptides
European Journal of Heart Failure 10 (2008) 70–77
Anwaruddin S, Lloyd-Jones DM, Baggish A, et al.
Renal function, con- gestive heart failure, and amino-terminal pro-brain natriuretic peptide measurement: results from the ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) Study.
J Am Coll Cardiol 2006;47:91–7.